Diplopia After Lower Orbital Floor Repair
Orbital Floor Blow Out Fractures

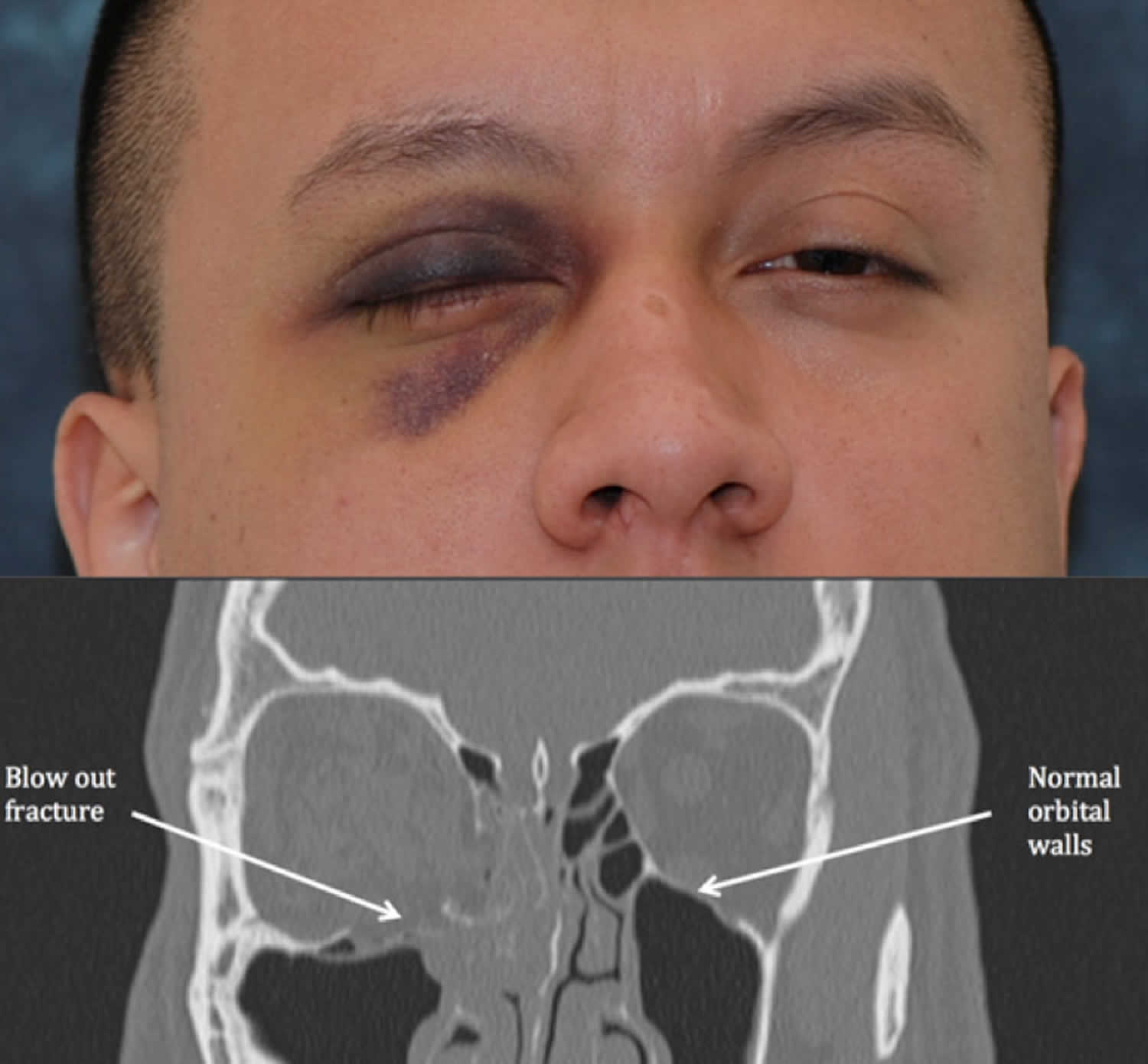
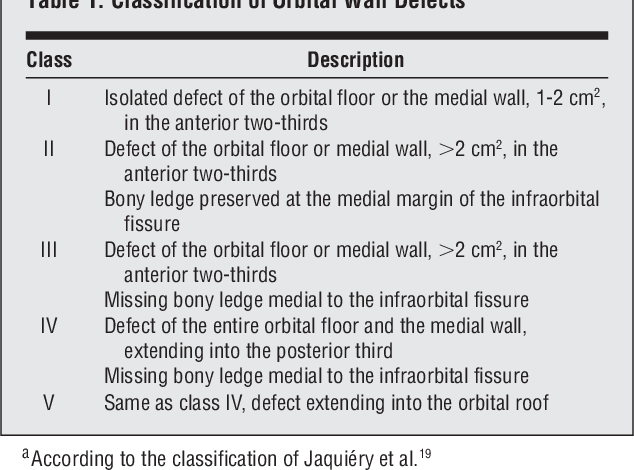
Orbital Blowout Fracture

Biomaterials And Implants For Orbital Floor Repair Sciencedirect
Orbital Floor Fracture Causes Symptoms Diagnosis Treatment Prognosis
.jpg)
Tamara Fountain Md

Transantral Orbital Floor Fracture Repair Using A Folded Silastic Tube

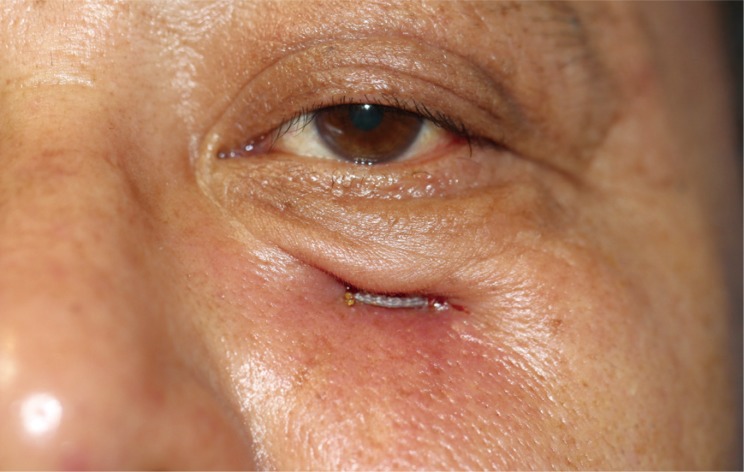
Adult patients who have diplopia or pain on eye movements in the acute setting of an orbital floor fracture should be evaluated again within a week following the injury and if diplopia persists should be seen at weekly intervals as long as the dysmotility is improving.
Diplopia after lower orbital floor repair.
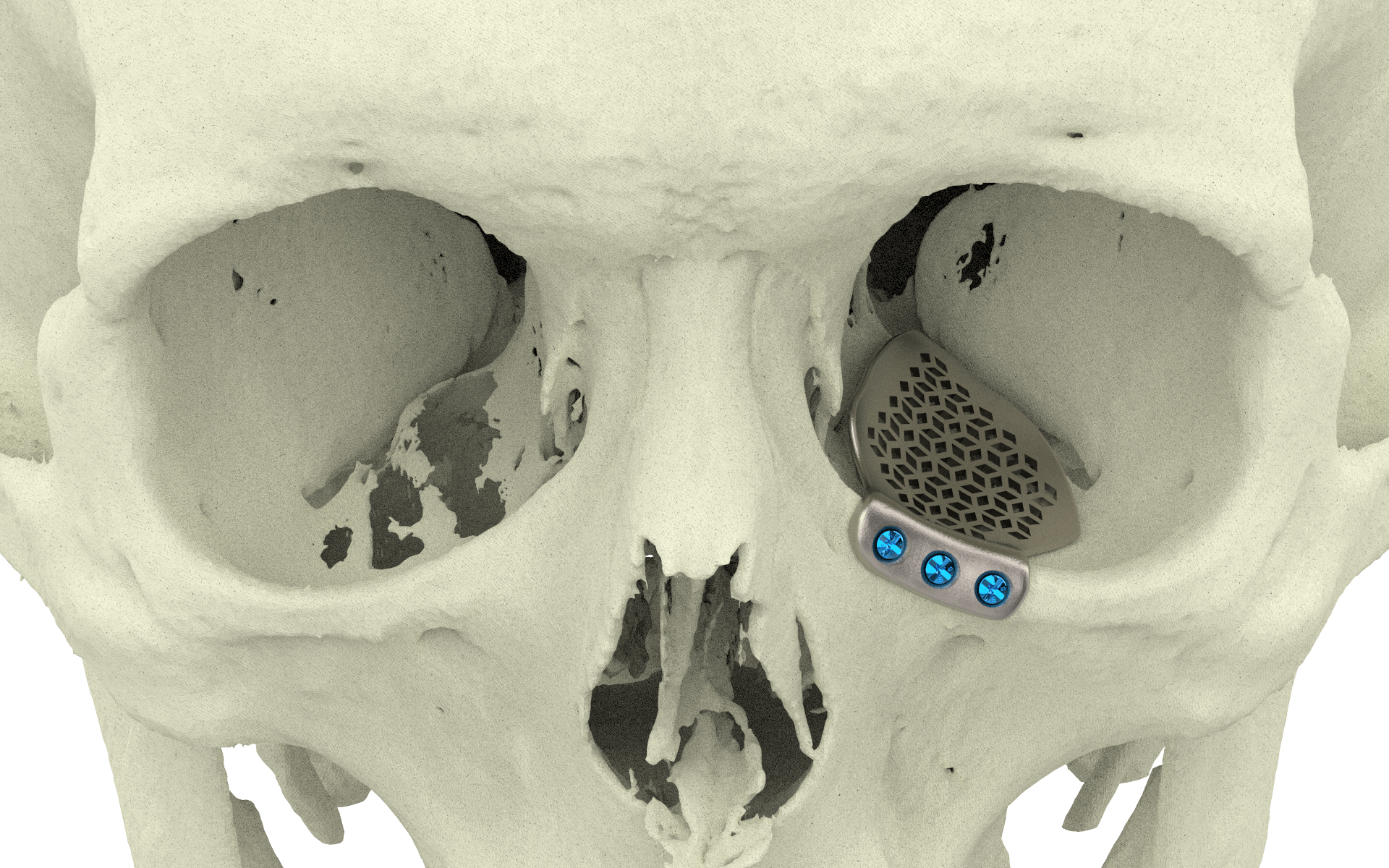
Orbital Floor Xilloc
Orbital Reconstruction For Orbit Medial Orbital Wall Fracture

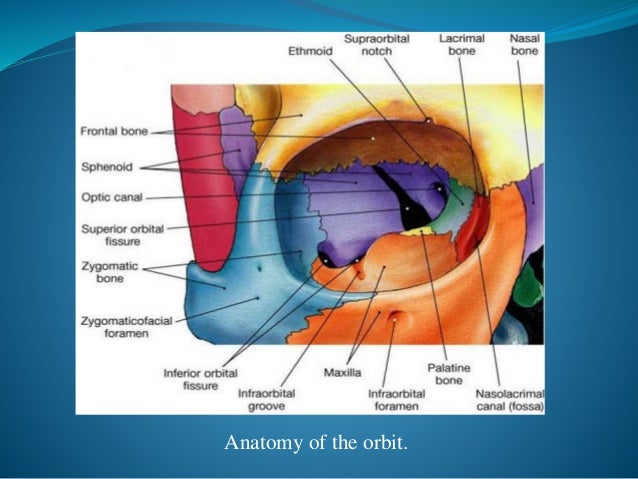
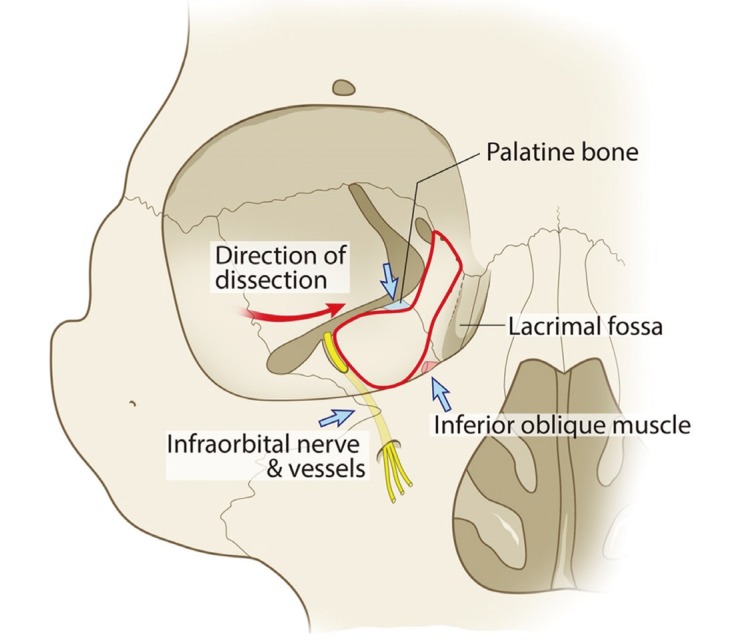
Bony Components Of The Orbital Floor Download Scientific Diagram
Pdf Repair Of Orbital Floor Fractures Our Experience And New Technical Findings

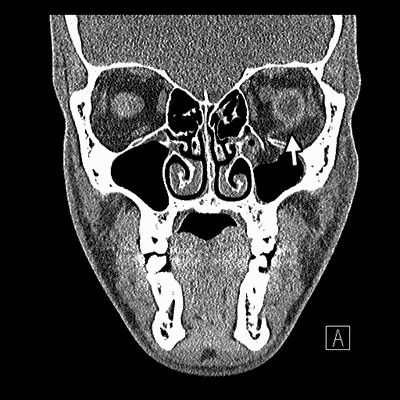
A Coronal Ct Scan Of The Patient Showing The Left Orbital Floor Download Scientific Diagram
Taking The Floor On Fractures
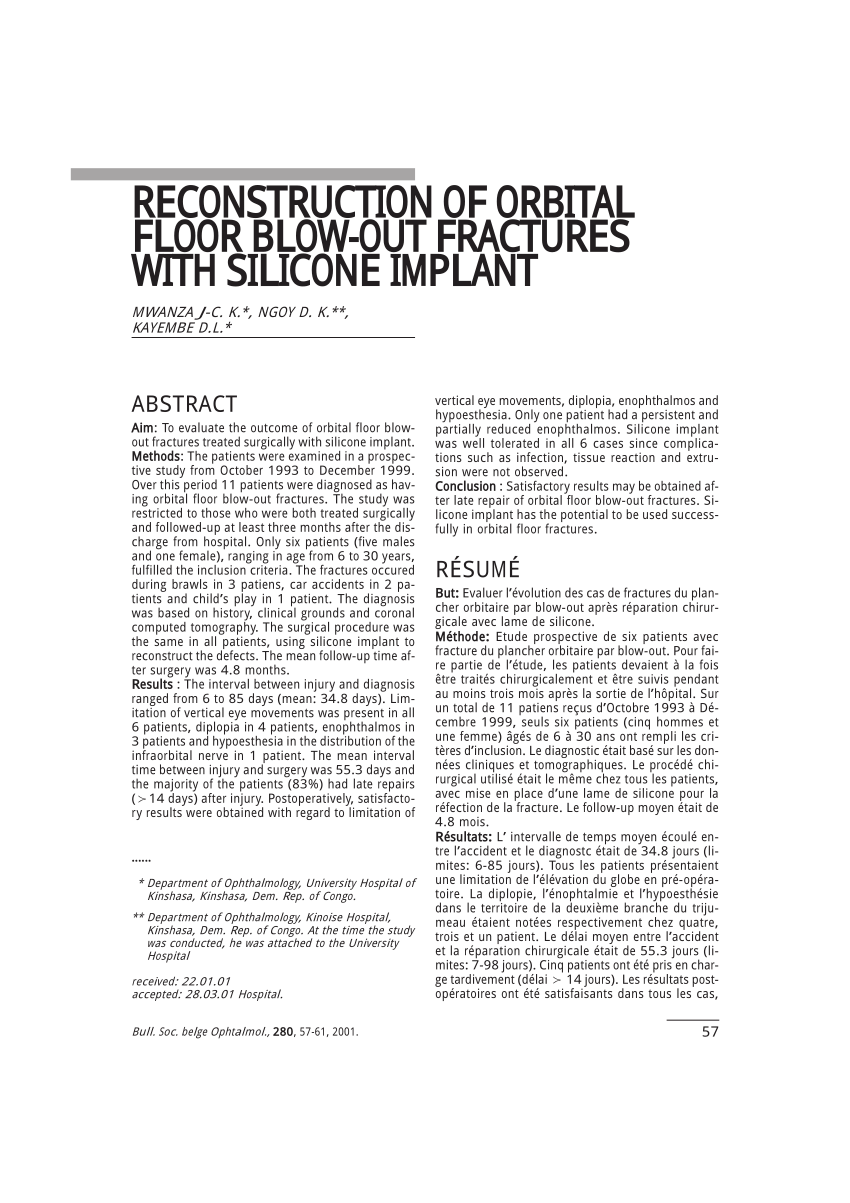
Pdf Reconstruction Of Orbital Floor Blow Out Fractures With Silicone Implant
Orbital Floor Fracture

Transconjunctival Approach To The Orbital Floor Download Scientific Diagram
Breast Cancer Andwhite Eyed Blowout Fracture Eyerounds Org Ophthalmology The University Of Iowa
Orbit Floor Fx Slides

Infraorbital Nerve Block For Isolated Orbital Floor Fracture Plastic And Reconstructive Surgery Global Open

Pediatric Orbital Fractures Abstract Europe Pmc

Type Of Grafts Used In Recontruction Of Orbital Floor Fractures Download Table

31 Orbital Floor Blowout Fracture Repair Ento Key

Brown Emergency Medicine
Pdf Repair Of Orbital Floor Fractures Using Bioresorbable Poly L Dl Lactide Plates Semantic Scholar

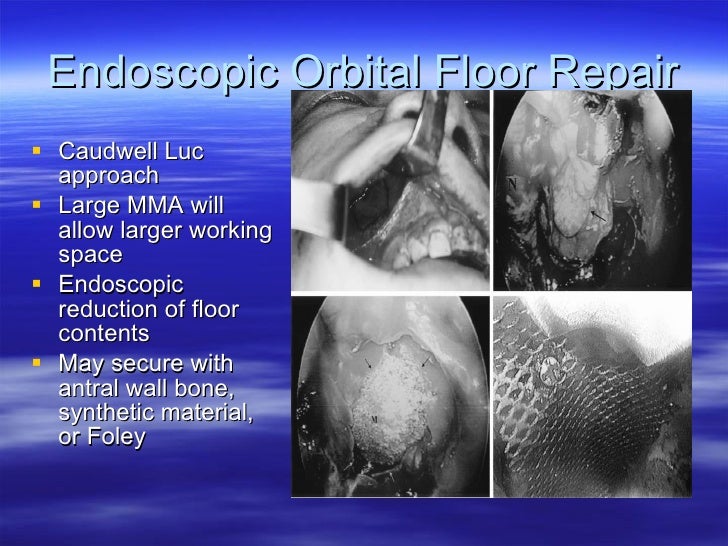
Endoscopic Transantral Repair Of Orbital Floor Fractures Sciencedirect
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcqycbcdgoe6rzb6oic0fdozorujti4io1tvpnsexbak2qbljwr3 Usqp Cau

Nhdogou2hzgx4m
Pdf Infraorbital Nerve Block For Isolated Orbital Floor Fractures Repair Review Of 135 Consecutive Cases
Biomaterials For Repair Of Orbital Floor Blowout Fractures A Systematic Review Semantic Scholar
Archives Of Craniofacial Surgery
Pdf Retroseptal Transconjunctival Approach For Blowout Fracture Of The Orbital Floor An Ideal Choice In East Asian Patients
Source : pinterest.com
